By
By - 138


Health Tips
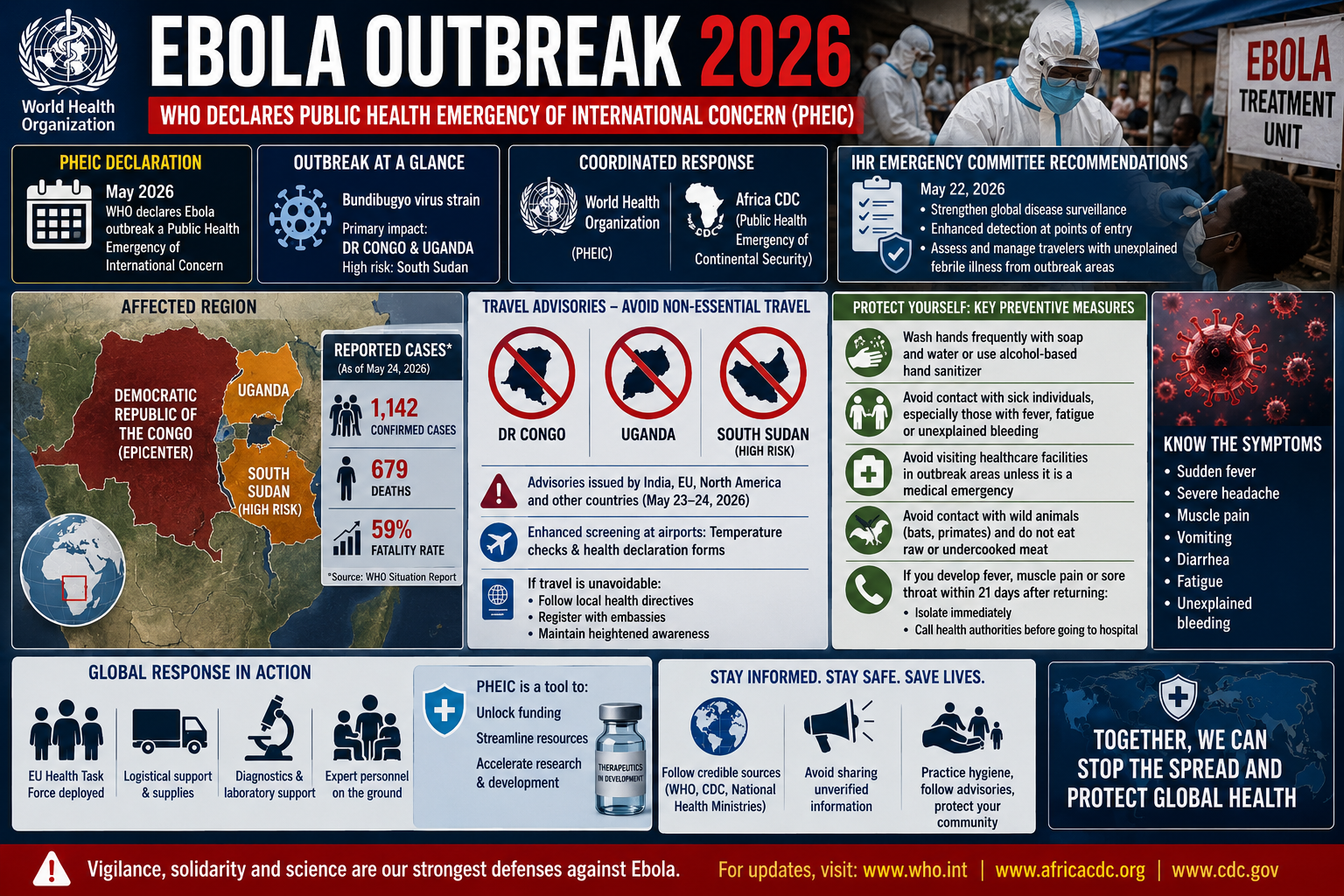
In a significant development for global public health, the World Health Organization (WHO) formally declared the ongoing Ebola disease outbreak in parts of Africa a Public Health Emergency of International Concern (PHEIC) in mid-May 2026. Driven by the Bundibugyo virus strain, this recent epidemic primarily impacts the Democratic Republic of the Congo (DRC) and neighboring Uganda, prompting swift action from international health monitoring bodies. Following the WHO's declaration, the Africa Centres for Disease Control and Prevention (Africa CDC) similarly escalated the situation to a Public Health Emergency of Continental Security. This coordinated categorization underscores the severity of the outbreak and the critical need for a unified global response to prevent further international spread. On May 22, 2026, the WHO’s International Health Regulations (IHR) Emergency Committee issued temporary recommendations aimed at strengthening disease surveillance globally, particularly at major points of entry. These guidelines emphasize the detection, assessment, and management of travelers presenting with unexplained febrile illnesses after arriving from documented outbreak zones. The immediate priority for health organizations worldwide is to contain the virus at its source while simultaneously preparing global health infrastructure for any potential imported cases, ensuring that medical professionals are equipped to handle the logistical and clinical challenges of a highly contagious pathogen.
As the situation evolves, governments worldwide have swiftly updated their travel guidance to protect citizens and mitigate the risk of cross-border transmission. Over the weekend of May 23–24, 2026, several national health ministries, including the Government of India, issued strict advisories urging citizens to avoid all non-essential travel to the DRC, Uganda, and neighboring South Sudan, which is currently assessed as being at high risk for disease transmission. Similar advisories are being echoed by health departments across Europe and North America, reflecting a consensus on the necessity of minimizing exposure. The European Centre for Disease Prevention and Control (ECDC) recently noted that while the current risk to the general public in regions like the EU remains very low, proactive measures are non-negotiable. International airports and global transit hubs are currently implementing enhanced screening protocols, including temperature checks and health declaration forms for passengers arriving from central and eastern Africa. For individuals whose travel to these regions is strictly unavoidable, authorities strongly mandate adhering to local public health directives, registering with their respective embassies, and maintaining a state of heightened operational awareness. This rapid tightening of international travel policies highlights the delicate balance governments must maintain: safeguarding domestic public health without imposing unnecessary restrictions that could cripple essential supply chains or humanitarian aid efforts in the affected regions.
For those navigating international travel during this global health alert, adhering to stringent personal hygiene and preventive health measures is the most effective line of defense. Because the Bundibugyo strain of the Ebola virus is transmitted through direct contact with the bodily fluids of an infected individual or contaminated surfaces—and currently lacks an approved vaccine or specific antiviral treatment—prevention relies entirely on avoiding exposure. Health experts advise travelers to practice meticulous hand hygiene, washing hands frequently with soap and water or using an alcohol-based hand sanitizer when soap is unavailable. It is crucial to avoid any physical contact with individuals showing symptoms of illness, particularly high fevers, fatigue, or unexplained bleeding. Furthermore, public health guidelines strongly caution against visiting healthcare facilities in outbreak areas unless it is a medical emergency, as these locations inherently carry a higher risk of transmission. Travelers are also instructed to avoid contact with wild animals, including bats and non-human primates, and to refrain from consuming raw or undercooked meat. If a traveler develops a sudden fever, muscle pain, or sore throat within 21 days of returning from a high-risk area, they must isolate immediately and contact local health authorities by phone prior to visiting a hospital, ensuring that medical staff can prepare the necessary infection control protocols before their arrival.
Moving forward, the trajectory of this outbreak will heavily depend on the efficacy of coordinated global interventions and the public’s adherence to evidence-based health advisories. The activation of international emergency frameworks, such as the deployment of the EU Health Task Force and ongoing surveillance by the WHO, represents a robust effort to provide logistical support, diagnostic resources, and expert personnel to the DRC and Uganda. While the classification of a PHEIC can understandably induce public anxiety, it is fundamentally an administrative mechanism designed to unlock international funding, streamline resources, and accelerate the development of potential countermeasures, including expedited research into targeted therapeutics. For the general public, the most responsible action is to remain informed through credible, authoritative sources such as the WHO, the CDC, and national health ministries, rather than relying on unverified information circulated on social media. Misinformation during a health crisis can lead to panic and the misallocation of vital resources. By practicing recommended hygiene standards, respecting travel advisories, and remaining vigilant about post-travel symptoms, individuals can play a direct role in safeguarding community health. Ultimately, transparent communication and collective adherence to public health guidelines remain the most powerful tools in navigating and eventually overcoming this international health emergency.